One of the first things I knew I wanted to write about almost four years ago when soundingsjohnbarker started was something about Samaritan’s Purse and the 2014 Ebola crisis, particularly in Liberia in West Africa. “A bigger picture” https://soundingsjohnbarker.wordpress.com/2014/09/03/a-bigger-picture/ became my third blog post here on Sept. 3, 2014.
It interested me because Samaritan’s Purse, a Christian international relief ministry run by Franklin Graham, son of the late North Carolina evangelist Billy Graham, and based in nearby Boone, North Carolina, was best known in recent years by many in North America for its Operation Christmas Child, which was started in 1990, and by 1993 it had grown to the point it was adopted by Samaritan’s Purse.
Samaritan’s Purse was founded by Dr. Bob Pierce in 1970 as a nondenominational evangelical Christian organization to provide spiritual and physical aid to hurting people around the world. Samaritan’s Purse Canada was established in 1973.
As of 2014, Operation Christmas Child had collected and distributed over 100 million shoebox gifts in more than 130 countries worldwide. Each shoebox is filled with hygiene items, school supplies, toys, and candy. Operation Christmas Child then works with local churches to put on age-appropriate presentations of the gospel at the events where the shoeboxes are distributed. Here in Thompson, hundreds of shoeboxes are collected each Christmas season for Operation Christmas Child through efforts co-ordinated in recent years mainly by the First Baptist Church, and previously the Thompson Pentecostal Assembly, which have co-ordinated efforts on behalf of a number of local churches, including St. Lawrence Roman Catholic Church, and other places including University College of the North (UCN), Thompson Public Library, and individual donors.
Rev. Leslie-Elizabeth King, who pastored the Lutheran-United Church of Thompson, and was in active ministerial service here for 19 years, until she retired in June 2014, touched a nerve in her “Spiritual Thoughts” column in the Nickel Belt News Oct. 26, 2012 when she mentioned using the Canada Revenue Agency website to look at how the Billy Graham Evangelistic Association of Canada’s Calgary-based Samaritan’s Purse Canada operates.
In a nutshell, while King had no problem with the charity’s six per cent management and administration budget expense, while 90 per cent went directly to the charity, which, she said, was “very good,” she didn’t much like the concept of sending shoeboxes stuffed with a pillowcase, toothbrush and a few pencils to a poor child on the other side of the world. “Wouldn’t it be better, if we truly want to be of use to others, to send our money to a church, agency or Non-Governmental Organization (NGO) in the destination country so local people could decide what is needed and where? That way, it would be more likely that our gift would build the economy in a community that needs it?” she asked.
Frank King, no relation, communications manager for the Billy Graham Evangelistic Association of Canada’s Samaritan’s Purse Canada, pointed out “our work in developing nations, including distributing Operation Christmas Child shoe box gifts, is always done through local partners. This is a priority for us because we want to build up local churches and we want to rely on local expertise to do (or financially support) the work that best benefits those communities.”
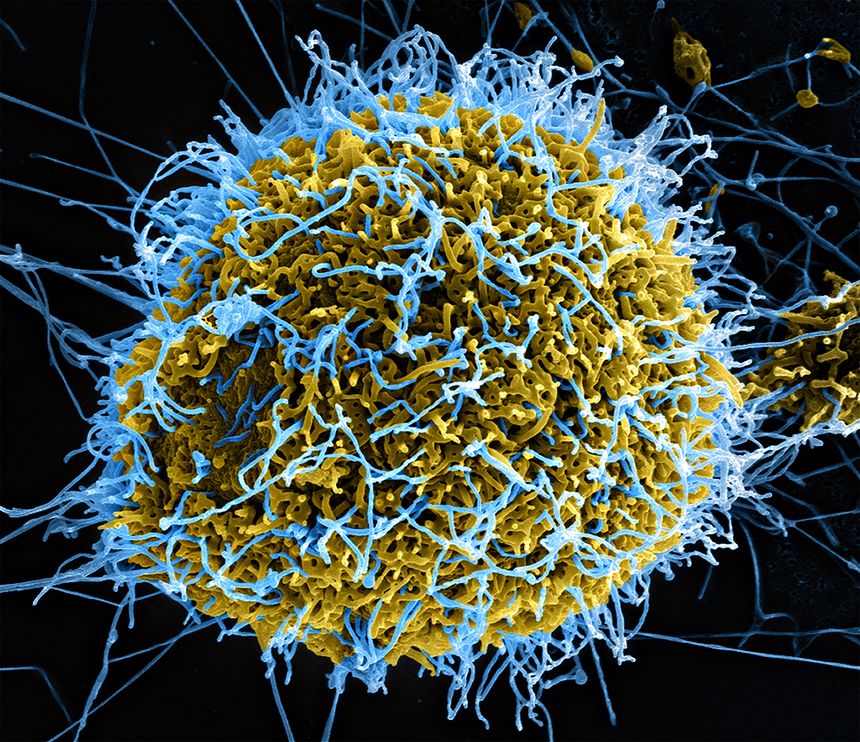
The Ebola story and Samaritan’s Purse was to me the international back story to the local Operation Christmas Child story. “Wouldn’t it be better, if we truly want to be of use to others, to send our money to a church, agency or Non-Governmental Organization (NGO) in the destination country so local people could decide what is needed and where?” Leslie King asked in 2012. Well, speaking of NGOs, in 2014 it would be Médecins Sans Frontières, also known in English as Doctors Without Borders, the highly respected international humanitarian medical non-governmental organization, founded in Paris in 1971, but stretched beyond their limits in Guinea and Sierra Leone in the midst of the deadliest Ebola viral hemorrhagic fever outbreak recorded in West Africa since the disease was discovered in 1976, that would ask Samaritan’s Purse on July 8, 2014 to take over the management of ELWA (Eternal Love Winning Africa) Hospital — the main facility, founded in 1965 by the medical mission group Serving in Mission (SIM) USA, caring for all Ebola patients in Monrovia, Liberia. The West African Ebola crisis — the world’s first urban outbreak as opposed to primarily rural previous ones — began in December 2013 in Meliandou, a small, isolated village in Guinea with only 31 households. It wasn’t until March 21, 2014, that the disease was identified as Ebola. The outbreak peaked in October 2014 and ended in June 2016.
Writing back in September 2014, what I knew then was that Dr. Kent Brantly, 33, medical director at Samaritan’s Purse Ebola Consolidated Case Management Center in Monrovia, contracted Ebola and was the first patient ever medically evacuated to the United States with a confirmed case of Ebola, to be treated at Emory University Hospital in Atlanta. Brantly originally moved to Liberia with his wife and children in October 2013 to be a general practitioner. Immediately after Samaritan’s Purse took over Ebola treatment operations in Liberia, he traded his hospital scrubs for a full-body hazmat suit.
I also knew that Brantly was the first Ebola patient ever treated with ZMapp, a highly experimental three-mouse monoclonal antibody drug serum treatment produced by U.S.-based Mapp Biopharmaceutical, based in San Diego. ZMapp was produced for Mapp Biopharmaceutical in the Reynolds American tobacco plant Kentucky Bioprocessing facility in Owensboro, Kentucky inside the leaves of tobacco plants. Two of the drug’s three components were originally developed at the Public Health Agency of Canada’s containment level 4 National Microbiology Laboratory (NML) in Winnipeg.
But what I didn’t know until I recently saw Samaritan Purse’s compelling 2017 documentary Facing Darkness on Netflix was that at the time Brantly was given ZMapp there were only four courses of ZMapp treatment in existence anywhere in the world. A specially-equipped isolation chamber Phoenix Air modified Gulfstream III air ambulance, the only one of its kind at the time in the world, chartered by Samaritan’s Purse to medically evacuate and repatriate Brantly, and en route from the United States to Liberia, had turned back half way across the Atlantic Ocean with a mechanical problem. Phoenix Air is headquartered in Cartersville, Georgia.
And then, a miracle by many measures. One of Brantly’s colleagues, and one of the physicians treating the critically-ill doctor, Dr. Lance Plyler, medical director of the Disaster Response Unit at Samaritan’s Purse, located one of those four courses of ZMapp in neighbouring Sierra Leone. A Styrofoam box containing three frozen vials of straw-colored fluid was flown to the border, canoed across a river and put on a plane to Monrovia, the Liberian capital. But there was enough to treat only one person, and meanwhile, Nancy Writebol, 59, with Serving in Mission, (SIM), had also contacted Ebola.
The day the ZMapp arrived in Monrovia, Brantly was actually having one of his better days since contracting the virus, and insisted that Writebol, who appeared sicker, be given the available ZMapp. But as the frozen vials were literally warming up under her arm, Brantly took a sudden and dramatic turn for the worse, and started to seize. Plyler made what must have required the Wisdom of Solomon-like Hippocratic Oath decision to retrieve the ZMapp vials from under Writebol’s arm, and administered the drug to Brantly instead. Brantly started to feel better almost immediately.
Both Brantly and Writebol would both wind up being treated with ZMapp and be medically evacuated by Phoenix Air within days, Brantly first, to Emory. Both made full recoveries.
Facing Darkness also provides insights into the character of Franklin Graham, as head of Samaritan’s Purse, that I had never seen before. While it may not be charitable to say so, in truth I have wondered more than once if Franklin Graham is up to being his father’s son. He’s a bit too of-this-world political and too cozy with President Donald Trump and his band of cronies for my taste. But recalling how he learned about Brantly contracting Ebola while he was in Alaska, Graham was almost ashen-face still as he recalled the moment. Speaking in the same measured tones Billy Graham often did, doesn’t take away from Franklin Graham’s sense of being overwhelmed by shock and grief. Initially, “I didn’t even know how to pray,” he says. But Graham would soon enough pray. And Samaritan’s Purse with Franklin Graham at the helm, would, in the best tradition of the United States Army Rangers nemo resideo, and “leave no one behind,” move heaven and earth to medically evacuate Brantly and Writebol from Liberia back to the United States.
A true-life page-tuner worthy of the best of the late Michael Crichton’s medical thrillers.
You can also follow me on Twitter at: https://twitter.com/jwbarker22